Hip Pain Relief · 7 min read · June 2026
Why most hip pain after 45 doesn't get better. And what an orthopedic hip surgeon is doing about it.
After 18 years operating on hips, I've come to believe most of my patients should never have been on my table. Here's what we've all been missing.
If you're reading this, your hip has probably been running your life for at least a year.
You sleep on your back, or on the good side, because rolling onto the bad one wakes you up at 3 AM with a deep ache on the outside of your hip. You brace before you get out of a chair. Getting out of the car is a production. The stairs have become the enemy. And turning over in bed, the simplest thing in the world, is the thing you dread most.
Some mornings you catch yourself walking like you're 84 instead of 54.
And picking up the grandkids, the one thing you always swore you'd be able to do, has quietly become something you line up and brace for.
You've already tried the obvious stuff.
Advil. Tylenol. A couple rounds of physical therapy at $75 a visit that loosened it up for a couple of days, then it locked right back. Maybe a cortisone shot that felt like a miracle for six weeks and then just stopped working. Maybe your doctor has started using the word "surgery," gently, the way they do.
And now you're stuck in the worst spot of all. Too sore to live like you used to. Not so far gone that you're ready to hand over four to six months of your life to a hip operation and the rehab that follows.
I've sat across from this woman more times than I can count.
"I just want it fixed. I'll book the surgery tomorrow if that's what it takes."
Last spring, Linda sat across from me. Fifty-eight years old, newly retired after twenty-two years running the front office at an elementary school. She'd been to three different doctors, two rounds of physical therapy, and one cortisone shot before she finally landed the referral to me.
I told her what I tell most women sitting in that chair.
Surgery for chronic hip pain after 45 is the last option, not the first.
And in her case, like in most cases, the real problem wasn't something that needed cutting.
It was a blood flow problem.
I want to walk you through what I mean, because if your hip has been giving you grief for the last year or two, what I'm about to explain has almost certainly never been said to you. Not by your doctor. Not by your physical therapist. Not by anyone who sold you a cortisone shot.
And maybe you've already collected the labels. Bursitis. Then it's your back. Then sciatica. Then "wear and tear, what do you expect at your age." Maybe an X-ray came back "normal" and you walked out feeling like a hypochondriac, like it was all in your head.
It was never in your head. And once you understand what's actually going on, the reason nothing has worked finally makes sense.
The hidden reason your hip won't heal
The gluteal tendons, the tissue on the outside of your hip that holds you steady every single time you stand, walk, climb a step, or roll over in bed, are some of the worst-fed tissue in your entire body.
Even in a healthy 25-year-old, they sit at the very edge of their blood supply. The tiny vessels feeding them are sparse compared to almost any other tissue you've got.
After 40, those vessels start to close.
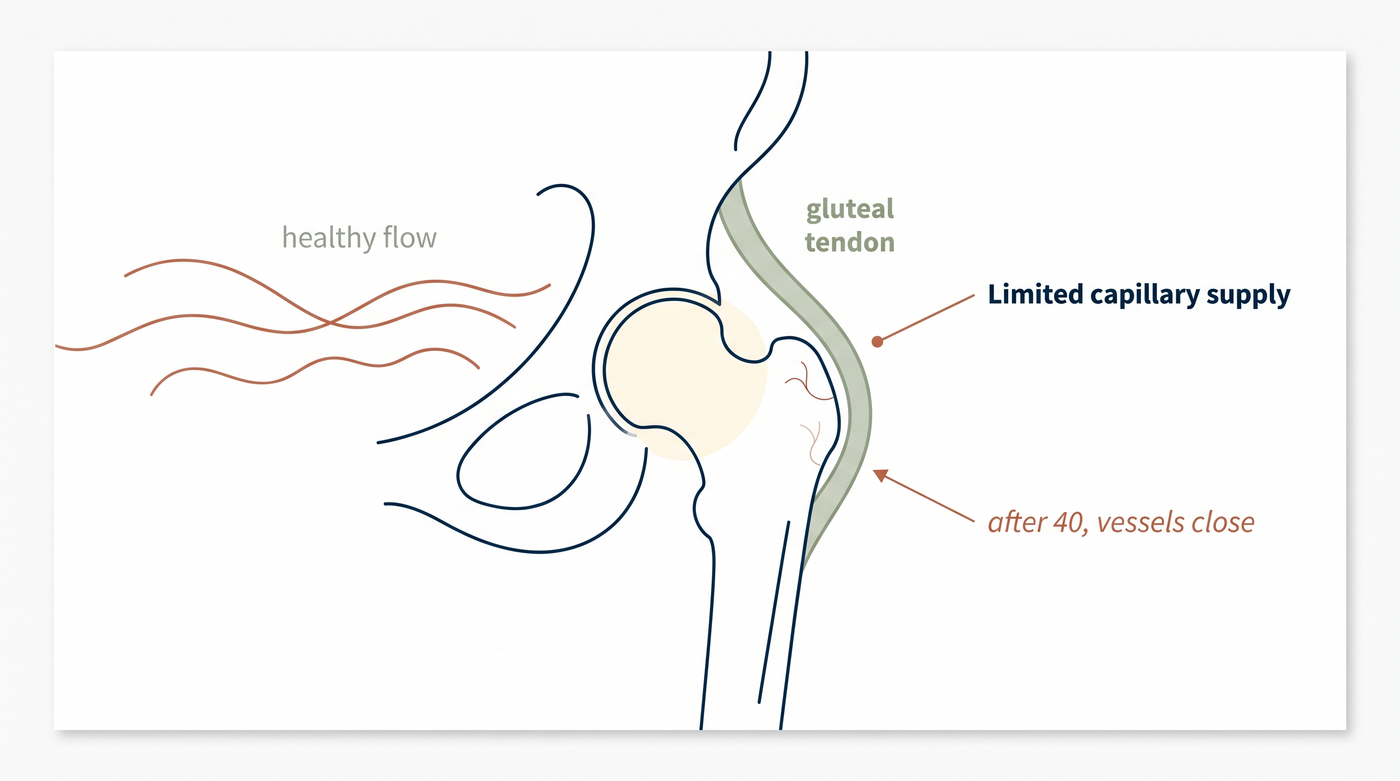
By your 50s, blood flow to these tendons can drop by 30 to 50 percent. By your 60s, it can be down as much as 70 percent. The tissue is still there. The structure is still there. But the supply line that keeps that tissue repairing itself, the oxygen, the nutrients, the machinery that clears out inflammation and rebuilds damaged fibers, has dried up.
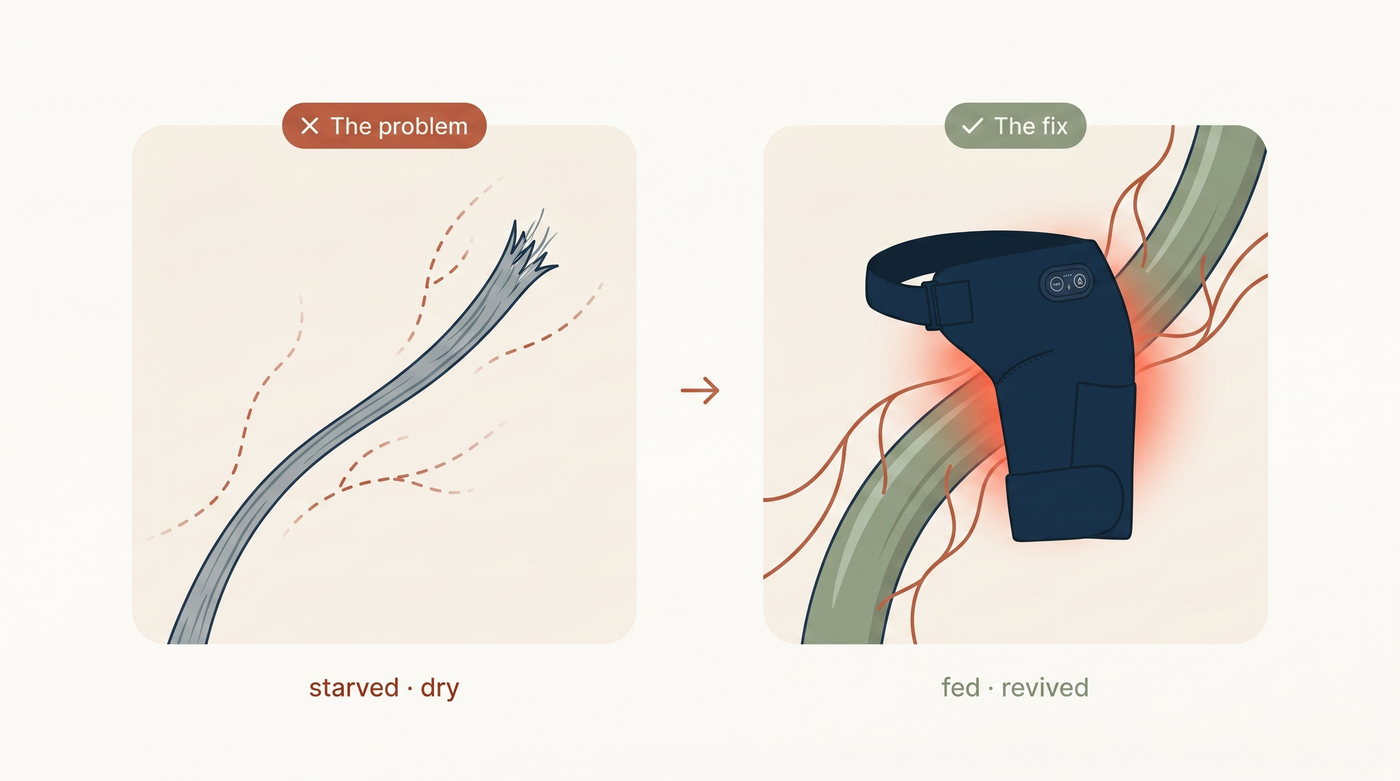
Clinicians call this hypovascular degeneration. In plain English: the tissue is starving.
And if you're a woman, there's a second hit your doctor almost certainly never connected to your hip.
Estrogen helps keep your tendons supplied and repairing. When estrogen drops in menopause, that already-thin blood supply drops further, and faster. It is not a coincidence that your hip started screaming around the same time everything else started changing.
You didn't wear your hip out. It's been quietly starving for years. And menopause cut off the last of its supply.
Here's what that actually does to you, day to day.
Every time you reach, stand, or take the stairs, you put tiny tears in that tendon. We all do, dozens of times a day. At 30, blood floods in and repairs them within hours. The machinery shows up. Job done.
The same tiny tear at 55? The blood doesn't show up. The repair doesn't happen. The damage compounds. The inflammation just sits there, because there's no flow to flush it out. And a hip that used to carry you without a second thought slowly becomes a stiff, aching, sleepless one.
Why everything you've tried hasn't worked
Once you understand the blood flow problem, the reason every common treatment fails becomes obvious.
Advil and Tylenol
They mask the pain signal. They don't restore one drop of blood flow. The pain comes back the second they wear off, because the actual cause was never touched.
Cortisone shots
They calm the inflammation locally, which feels miraculous for about six weeks. But cortisone weakens tendon tissue with repeated use, and it does nothing about why the inflammation was there in the first place.
Physical therapy
It strengthens the muscles around the hip and helps your range of motion. That has real value. But your physical therapist cannot rebuild the blood vessels you've lost.
Heating pads
They warm the skin and the surface. But your gluteal tendons sit deep. A heating pad feels nice for ten minutes. It is doing almost nothing to the tissue that actually needs help.
A red light wrap on its own
It can reach the cells, but it can't move the blood that starving tissue needs delivered first.
Surgery
It addresses the structural damage. It does not address why the tissue broke down in the first place.
The reason none of these worked isn't that you did them wrong. It's that the tissue was already starving. And not one of them feeds it.
What actually helps
The real answer to chronic hip pain after 45 isn't to cut anything. It's to restore blood flow to the tissue, so it can finally do what it was built to do: repair itself.
And restoring blood flow to a starving tendon takes four things working at once. This is the part no single device, and no heating pad, has ever done.
107°F Precision Heat · Open the vessels
Reopen the supply line
Not a hot water bottle. Sustained, regulated heat at the upper end of the safe range penetrates past the skin into the deep tendon and dilates the capillaries that have been closing for years. The vessels open. Blood starts moving again.
Rhythmic Compression · Flush and feed
The pump your tendon lost
Pressure that cycles on and off pushes the stale, inflammatory fluid out of the joint and draws fresh, oxygen-rich blood in to replace it.
Targeted Massage · Reach the deep tissue
Go where heat can't
Deep massage loosens the stiffened tissue that's built up over years of guarding, breaks down the adhesions that lock your hip, and wakes up the repair signal.
Red Light Therapy · Power the cells
Make the cells burn the fuel
Red and near-infrared light reaches the tendon and switches the cells' own energy back on, so the tissue can actually use the blood you just restored to rebuild. Heat and compression deliver the fuel. Red light makes the cells burn it. This is the piece a massage gun, a heating pad, or a red light panel on its own will never give you.
And here's what we'd all been missing.
All four have to run together. In one session. At the same time.
Heat opens the vessels but doesn't power the cells. Compression moves the fluid but can't open vessels that have been shut for years. Massage reaches deep, but the tissue can't use it with no blood and no energy. Red light fuels the cells, but only once the blood is delivered.
That's why the heating pad did nothing. Why the pills did nothing. Why the red light wrap on its own did nothing. Each one was doing a single piece of a four-piece job.
Run all four together, 15 minutes a day, and the tendon finally gets everything it's been starved of. At once.
The recovery arc most of my patients see
15 minutes a day. What changes, and when.
All timing below is illustrative — substantiate before publishing.
The device I now recommend before surgery
About 18 months ago, after watching too many women sit in my office hoping I could undo what biology had spent twenty years quietly doing, I started working with a team of biomedical engineers on something different. A device that could deliver all four therapies, heat, compression, massage, and red light, in a single 15-minute session, at home.
INTRODUCING
Mendable Hip
4-in-1 Therapy System · 15 minutes a day

It's a wrap that straps around the hip. One control unit, one button to start. It runs all four therapies together for exactly 15 minutes, then shuts off on its own. You do it once a day, in your own living room, while you watch TV or have your coffee.
I started recommending it last year to the women I genuinely believed should not be rushed into surgery. Women like Linda.

Linda used Mendable Hip once a day for six weeks before her next appointment with me.
When she came back, she didn't say anything at first. Then she stood up out of the chair, smoothly, no hands, no bracing, and looked at me.
"I haven't gotten up like that in two years. I cancelled the surgery."
She hasn't rebooked it.
And she's not the only one. Of the women I've recommended Mendable Hip to over the last twelve months, women who walked in expecting me to schedule an operation, most have not gone on to have one. Some still will. Some genuinely need surgery, and Mendable Hip is not going to change that. But for the rest, the women in their 50s and 60s whose hip simply needed feeding again, it has done what physical therapy and cortisone never could.
It fed the tissue.
What Mendable Hip is, and what it isn't
Mendable Hip is not a cure. It is not a replacement for surgery when surgery is genuinely necessary. It is not a magic device.
It is a clinical tool. Four established therapies delivered together, daily, at home, for the kind of chronic, slow-onset hip pain where the real problem is a tissue that stopped getting fed, not an injury that needs cutting.
For the women I see, in their 40s, 50s, and 60s, with the won't-go-away lateral hip pain that started around menopause, that physical therapy can't quite fix and cortisone only masks, it has changed how I practice.
It's designed in the US. It ships from a US warehouse. And it comes with a 90-day money-back guarantee.

COMPLETE RECOVERY PACKAGE
Mendable Hip Therapy System — 4-in-1
GET YOURS 50% OFF →NOT AVAILABLE ON AMAZON OR EBAY
- ✓Mendable Hip 4-in-1 Therapy Device
- ✓Premium Carrying Case
- ✓3 FREE Guides ($87 Value)
- ✓Quick-Start Guide
- ✓FREE US Priority Shipping
- ✓90-Day Money-Back Guarantee
- ✓Unlimited Customer Support
A fair shot. The full window for real change.
Use Mendable Hip daily for 90 days. If your hip isn't sleeping better, moving better, and getting up easier, every cent comes back. No forms. No store credit. No runaround.
If your doctor has started saying the word "surgery," and you haven't booked it yet, Mendable Hip is what I'd ask you to try first.
It's the option that goes before the operating room. It gives the tissue a chance to repair itself, while you still have that chance.
Most of the women I see tell me they wish they'd known about it a year ago.
If that's where you are right now, this is where to start.
Dr. Michael R. Callahan, MD, is a board-certified orthopedic hip surgeon based in Denver, CO, specializing in gluteal tendinopathy, greater trochanteric pain syndrome, gluteus medius and minimus tendon repair, and hip preservation. He has performed more than 2,000 hip procedures over his career.